ENDODONTICS AND ESTHETIC DENTISTRY(12)
Access Cavity Preparation
An access cavity must be large enough to enable proper debridement of the entire chamber and canal system yet small enough to preserve tooth structure. Discoloration from retained pulpal tissue and/or filling materials must be prevented. Therefore, chamber access must be internally widened and all pulp horns unroofed. A fine line exists between protection of existing restorations and tooth structure and a sufficiently sized access cavity to achieve the desired endodontic result.
A carefully planned and executed access cavity preparation should minimize weakening the tooth, provide for maximum visibility, and allow for straight line access into all root canals for optimal preparation and filling of the canal(s) (Figure 19-44).

Figure 19-44: Straight line access allowed for visualization of all four canals in the maxillary second molar.
Entering the pulp chamber requires a general knowledge of tooth morphology, the specific intricacies of the tooth in question, and proper instrumentation. Recent radiographs that were taken with a paralleling device to ensure minimal distortion should be studied prior to picking up the handpiece. It is recommended that two preoperative films be exposed from different horizontal angles to provide better information and help in visualizing the crown and root morphology (see Figures 19-24A and B).
The films should depict the location of the chamber, presence or absence of calcification, number of roots and canals, and relationship of the incisal or occlusal surfaces to the axial line of the root.
Morphologically, the access cavity takes the shape of the underlying pulp chamber (Figures 19-45A to C). Variations in size and shape of the pulp chamber take place as the result of calcification resulting from caries, operative procedures, restorations, occlusal wear, abrasion, etc. Therefore, by nature, the access cavity in a youngster's nonrestored tooth (Figures 19-46A, and 19-46B) would differ considerably from that of the same tooth with multiple restorations in a middle-aged person (Figures 19-47A, and 19-47B).
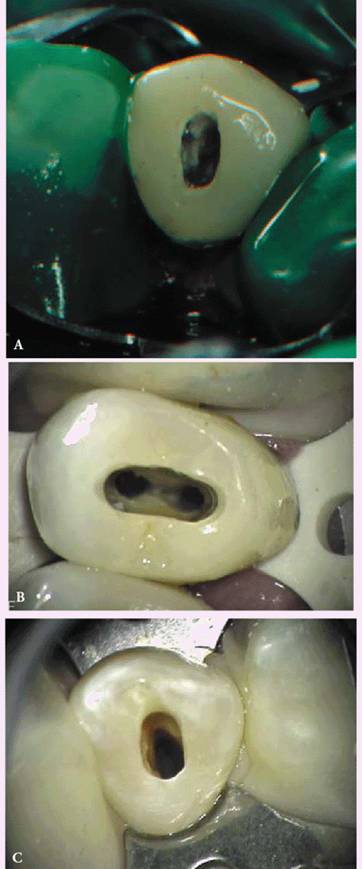
Figure 19-45A to C: Access cavity outlines reflect the shape of the pulp chambers: (A) maxillary canine, (B) maxillary premolar, and (C) mandibular premolar.
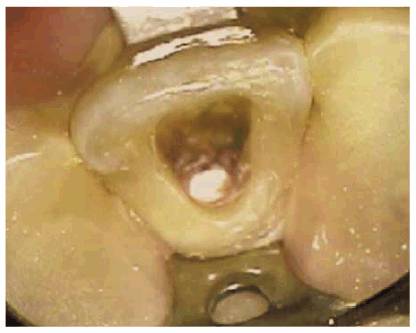
Figure 19-46A: Access cavity in a traumatized unrestored maxillary central incisor of a 16-year-old male.
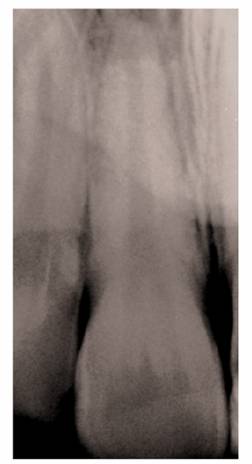
Figure 19-46B: Radiograph of the same tooth showing a large pulp chamber and root canal.
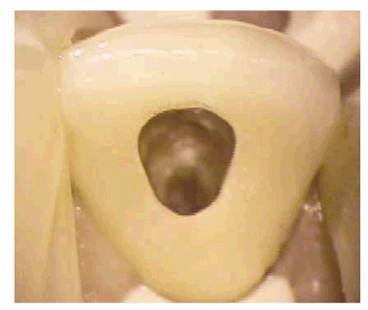
Figure 19-47A: Access cavities through porcelain-fused-to-metal crowns in a middle-aged male.

Figure 19-47B: Radiograph of the same tooth depicting a narrow root canal. The size of the access opening in the crown reflected the recession of the pulpal complex.
Magnifying loupes or a dental operating microscope are necessary aids in searching for canals when calcification has obliterated the chamber. Magnification in conjunction with an auxiliary light source tends to reduce the frustration of this phase of endodontic therapy.
- on 01.11.2012 [endodontics]
- on 01.11.2012 [endodontics]
- on 01.11.2012 [endodontics]
- on 10.13.2011 [endodontics]
- on 12.15.2010 [endodontics]
- on 08.11.2010 [endodontics]
- Long Island College Hospital - [education]
- Faculty of Dental Medicine - H [education]
- The American Association of Or [organize]
- Summer Institute in Clinical D [organize]
- Academy of Osseointegration [organize]
- University of North Carolina a [education]
- American Orthodontic Society [article]
- American Equilibration Society [article]
- Niigata University - Japan [education]
- University of Buffalo [education]